Case30
●1979
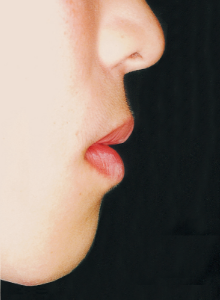
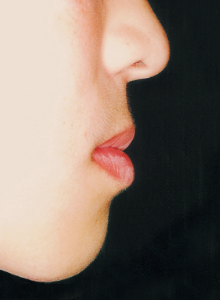
Age at Initial Visit: 8 years 1 month, Female / Protruding lower bite. Protruding lower jaw
Active Treatment Period: 1st Phase Treatment: 2 years 5 months
2nd Phase Treatment: 1 year 8 months
Non-extraction / Surgery
Age at Initial Visit: 8 years 1 month, Female / Protruding lower bite. Protruding lower jaw
Active Treatment Period: 1st Phase Treatment: 2 years 5 months
2nd Phase Treatment: 1 year 8 months
Non-extraction / Surgery






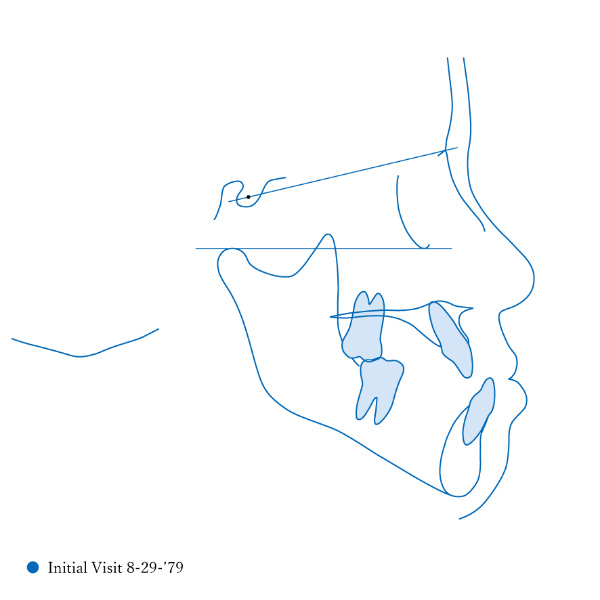
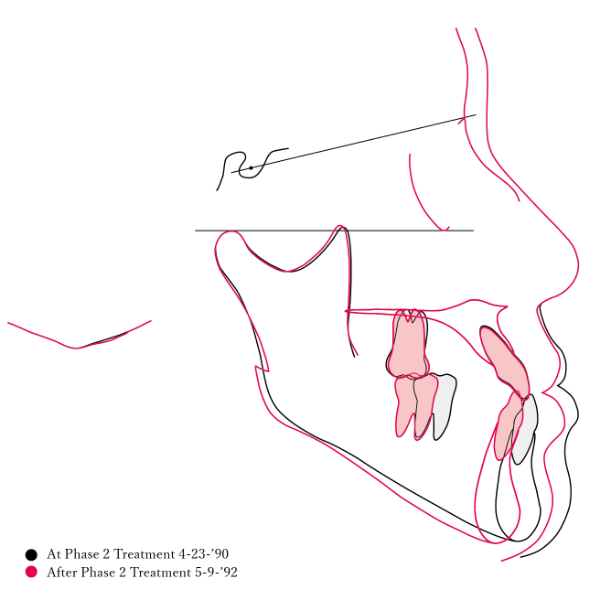
1 Initial Visit 8-29-’79





2 After Phase 2 Treatment 5-9-’92
A case raising questions about the limits of orthodontic treatment and the significance of early treatment.
This case presented with Class III malocclusion and significant negative overjet from the early mixed dentition. Regular observation was conducted, and Phase I treatment was initiated after the eruption of the anterior teeth, improving the anterior occlusal relationship and molar relationship. Subsequently, regular observation continued toward the completion of the permanent dentition. However, due to vigorous mandibular growth, orthodontic treatment including surgery became necessary.
This case presented with Class III malocclusion and significant negative overjet from the early mixed dentition. Regular observation was conducted, and Phase I treatment was initiated after the eruption of the anterior teeth, improving the anterior occlusal relationship and molar relationship. Subsequently, regular observation continued toward the completion of the permanent dentition. However, due to vigorous mandibular growth, orthodontic treatment including surgery became necessary.
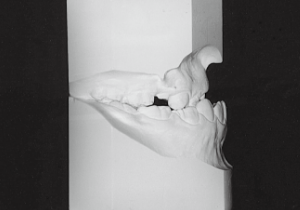
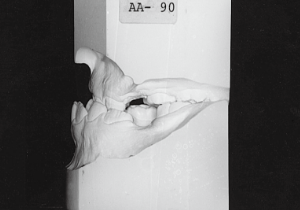
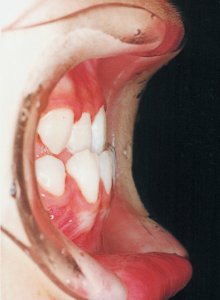
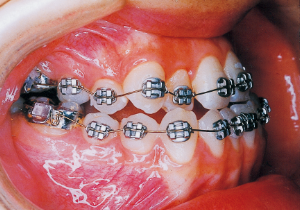
3 Initial Visit 8-29-’79
3 Initial Visit 8-29-’79
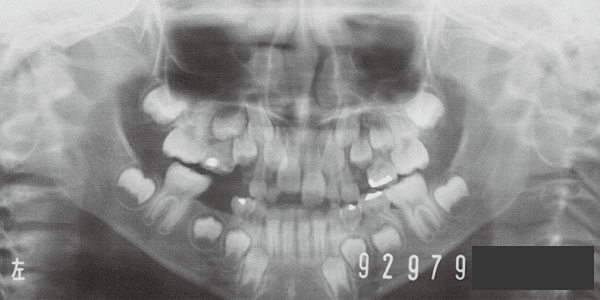
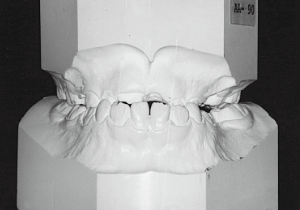
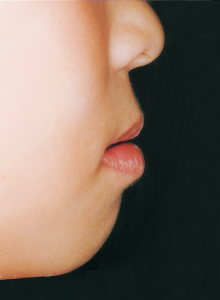
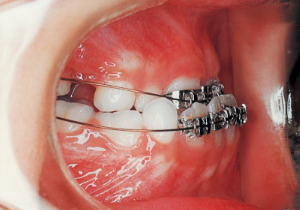
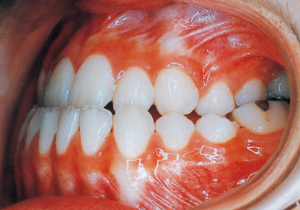
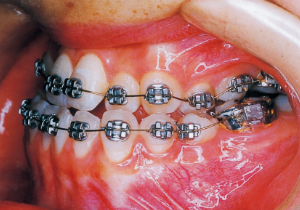
4 Initial Visit 8-29-’79
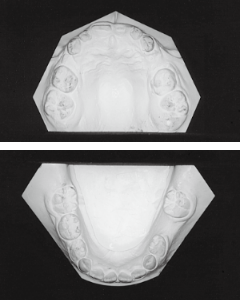
5
Although there were many missing deciduous teeth, the number of permanent teeth was not problematic (4). The amount of negative overjet was significant (1). On cephalometric radiographs, the mandibular ramus was not relatively long, but the large gonial angle and the long mandibular body were noticeable, indicating an overall tendency of the mandible to project inferiorly and anteriorly. High lower facial height was also characteristic.
A potential predisposition to mandibular protrusion was clearly evident.
A potential predisposition to mandibular protrusion was clearly evident.


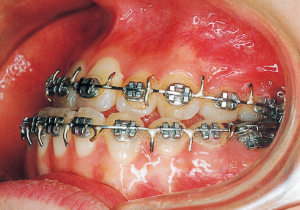
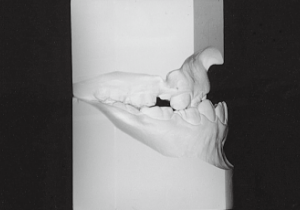
6 8-29-’79 Initial Visit 8 years and 1 month old

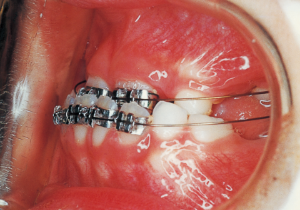
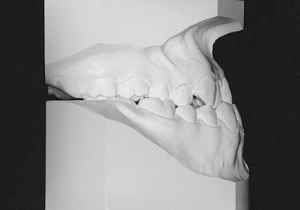
7 1-22-’80 Beginning of first phase


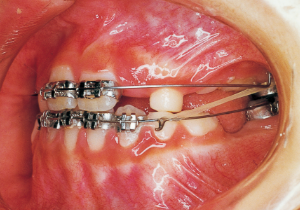
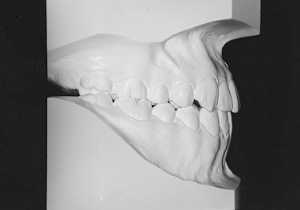
8 1-20-’81 One year after start of treatment




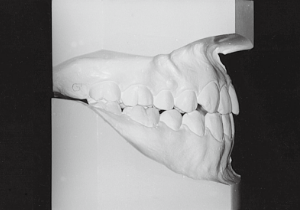
9 7-28-’82 After Phase 1 Treatment 11 years old
Aware that treatment would be challenging, we proceeded with the first phase of treatment based on the current functional status and anticipated developmental implications (7). During the mixed dentition phase, the body responds readily to treatment, allowing for relatively rapid tooth movement and changes in jaw position (8,9). Subsequently, once freed from mechanical stimulation, growth continues according to inherent predispositions, often appearing to disregard occlusal functional efficiency (10,11). These changes are clearly observable on cephalometric radiographs (12). After confirming the extent and direction of growth, we decided to incorporate surgical intervention into the treatment plan and wait until the age when growth begin to decline.



10 6-25-’84 During observation 12 years and 11 months old


11 9-28-’85 During observation 14 years and 2 months old
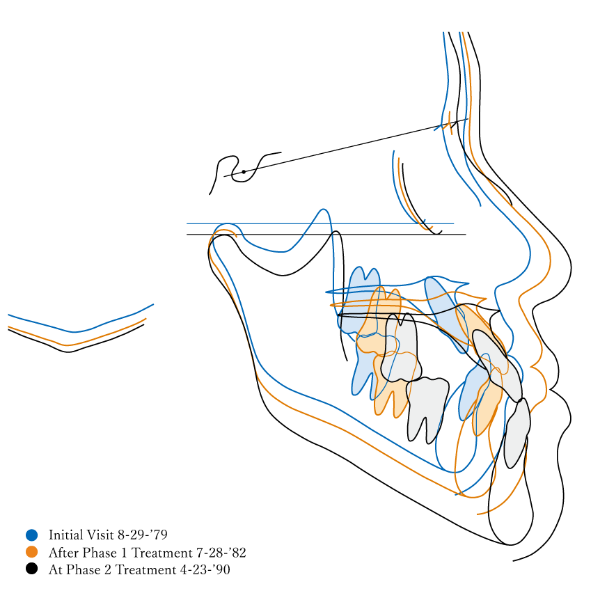
12





13 5-21-’90 At Phase 2 Treatment

14 6-21-’90 Beginning of second phase


15 3-23-’91 Before surgery



16 5-9-’92 After Phase 2 Treatment



17 8-15-’94 After Retention 14 years and 7 months after start of treatment
First Phase treatment: Treatment continued for a long period of 2 years and 5 months, from age 8 years and 6 months to age 10 years and 11 months.
Afterwards, follow-up was conducted, but based on the growth pattern, surgical intervention was determined necessary, and the patient entered a period of regular observation.
Regular Observation: 8 years from 10 years 11 months to 18 years 11 months
Second Phase Treatment:
Pre-surgical orthodontic period: 9 months
Hospitalization period: 2 weeks
Intermaxillary fixation period: Approximately 1 month (orthodontic treatment was not possible during this period).
Post-surgical orthodontic period: 10 months
Retention period: 2 years 5 months
Total Management Period: 15 years from 8 years 1 month to 23 years 1 month
Afterwards, follow-up was conducted, but based on the growth pattern, surgical intervention was determined necessary, and the patient entered a period of regular observation.
Regular Observation: 8 years from 10 years 11 months to 18 years 11 months
Second Phase Treatment:
Pre-surgical orthodontic period: 9 months
Hospitalization period: 2 weeks
Intermaxillary fixation period: Approximately 1 month (orthodontic treatment was not possible during this period).
Post-surgical orthodontic period: 10 months
Retention period: 2 years 5 months
Total Management Period: 15 years from 8 years 1 month to 23 years 1 month
8-29-’79 Initial Visit

7-28-’82 After Phase 1 Treatment
5-21-’90 Before Phase 2 Treatment
5-9-’92 After Phase 2 Treatment
8-15-’94 After Retention
18
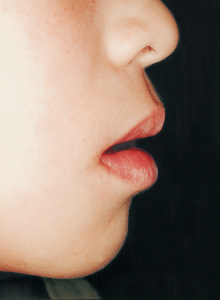
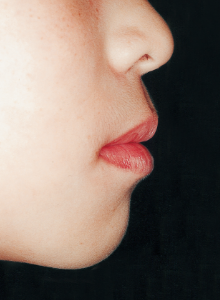
Reflecting on the course of treatment, one cannot help but marvel at the strength of the inherent biological program. At the same time, it makes one ponder how much artificial influence the body can allow and adapt to. While it would be difficult to say the long-term work in the first phase was suddenly meaningless, we must consider how much value it held for the overall treatment. The tongue is always positioned low due to its anatomical relationship within the facial structure. While it is understood that this low tongue position affects the dental arch, current treatment methods offer no solution. In such cases, we are acutely aware of the limited scope of what we can do.